
Leslie Quiwa, MD, FPCP, FPCEDM
As the year 2022 comes to a close, the most recognizable disease worldwide is COVID-19. While diseases like diabetes mellitus or hypertension are surely familiar to many, the pandemic’s impact has been profound. Confronted with this threat, massive research articles on COVID-19 have been published, accompanied by record-breaking speed in the development of vaccines.
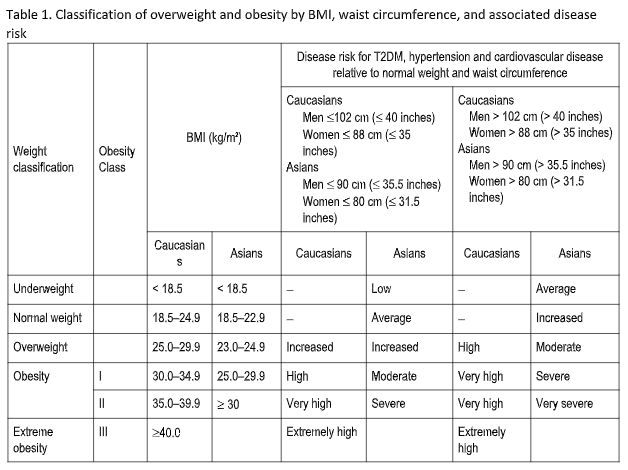
It is recognized that obesity increases the risk for severe disease and higher mortality from COVID-19. The World Health Organization (WHO) defines obesity as abnormal or excessive fat accumulation that presents a risk to health. In clinical practice body mass index (BMI) is often used to define obesity, and the corresponding cutoffs are ≥ 30 kg/m2 and ≥ 25 kg/m2 for Caucasian and Asian populations, respectively (Table 1). The difference reflects the fact that Asian populations develop obesity-related complications at lower BMIs, with a tendency to accumulate intra-abdominal fat without developing generalized obesity. In obese COVID-19 individuals several mechanisms have been implicated as the drivers of increased morbidity and mortality. These include immune dysfunction, adipose tissue inflammation and insulin resistance-induced metabolic alterations, comorbidities and organ failures including respiratory dysfunction with obstructive sleep apnea.
In 2021, the European Society for Clinical Nutrition and Metabolism (ESPEN) has endorsed some statements on ways to mitigate the effects of COVID-19 among persons with obesity. Here we summarize these to give an overview of the topic. The full-text of the recommendations is available here: https://doi.org/10.1016/j.clnu.2021.05.006.
There are varying recommendations for weight-based calorie requirements, especially in the ICU. Although in the most recent ICU guidelines, ESPEN suggests to calculate energy requirement using the utilization of Adjusted Body Weight:
(ABW = Ideal Body Weight + 25% Excess Body Weight)
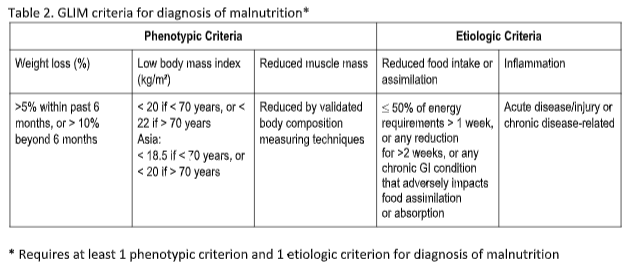
Persons with obesity require early intervention and screening for malnutrition risk using validated tools, especially among those with additional risk factors or comorbidities. An example of a validated tool is MUST, accessible at https://www.bapen.org.uk/screening-and-must/mustcalculator. This screening does not require the expertise of nutrition specialists and thus can be widely implemented to readily identify high-risk individuals. Once these persons are identified they should undergo diagnostic assessment using validated tools. The Global Leadership Initiative on Malnutrition (GLIM) criteria for simple malnutrition diagnosis can be used and has been recently published in a consensus paper by all major global nutrition societies (Table 2). Other validated tools for comprehensive nutritional assessment to diagnose malnutrition in the outpatient setting include SGA and MNA for geriatric populations.
Optimizing the nutritional status of persons with obesity is ideally achieved through the support of experienced healthcare professionals. The team must include dietitians, clinical nutritionists and medical specialists. However, some general guidance can be provided that will benefit any clinician handling these patients. With regard to protein intake, a reasonable approach is to provide at least 1 g of protein /kg ABW per day in the absence of chronic kidney disease.
In computing for caloric requirements, 25 kcal/kg ABW per day is recommended unless weight loss is indicated. The decision to promote weight loss should be based on a careful risk-benefit assessment, and any intervention should aim for a slow, gradual weight loss to minimize loss of skeletal muscle mass, using balanced diets with limited calorie deficits up to 500 calories/day.
Diet plans should ensure appropriate amounts of complex carbohydrates and dietary fiber, limit saturated fat and increase the dietary content of mono- and polyunsaturated fatty acids.
Oral nutritional supplements (ONS) can also be considered when dietary intake is not sufficient to meet calorie and protein targets, especially for older adults and those with multiple comorbidities. Dietary allowance of vitamins and other micronutrients should also be ensured since persons with obesity are also at risk for micronutrient deficiencies, particularly in the presence of malnutrition.
If a person with obesity is hospitalized for COVID-19 and oral intake including ONS is not sufficient to meet nutritional targets, then enteral nutrition (EN) should be started. If this is contraindicated or not sufficient to meet targets parenteral nutrition (PN) can be started. Protein and calorie requirements are suggested to be > 1g/kg ABW per day and 25 kcal/kg per day respectively. These patients should have enough vitamins and micronutrients with oral diet or medical nutrition treatments to meet the recommended daily allowance. For patients with diabetes, Diabetes-Specific Formula (DSF) may be considered, especially when glucose control is poor, whose values are above 180 mg/dL.
Obese individuals with COVID-19 are at higher risk of admission in the ICU. If these individuals are not intubated and admitted to the ICU, ONS or EN treatment should be started, if indicated, to reach protein and energy targets. PN should be considered if oral and enteral treatment are contraindicated or insufficient to reach targets. If the patient is intubated, EN should be started gradually to reach energy targets while ensuring high protein delivery. It should be recognized that using a prone position is not by itself a contraindication for EN. An initial calorie target of 20 kcal/kg ABW per day is reasonable. and this Hypocaloric feeding aims to avoid overfeeding and its associated metabolic and clinical risks during the hyperacute ICU phase. Subsequently, calories can be gradually increased up to estimated isocaloric needs of approximately 25 kcal/kg ABW per day after the first week, following individual evaluation. For protein targets, it is recommended to give at least 1.3 g/kg ABW per day. Nutrition formulas for ICU patients should provide high calorie density (1.5 kcal/mL) and high protein content. However, since a significant number of obese patients admitted in the ICU have pre-existing metabolic syndrome or T2DM, strict glucose control protocols should be implemented to avoid severe hyperglycemia of > 180 mg/dL. Once these patients are extubated, oral nutrition should be reintroduced to reach nutritional targets. If post-extubation dysphagia is present, texture-adapted food should be administered or EN should be considered when swallowing is unsafe because of aspiration risk.
When feasible, persons with obesity should be provided with opportunities for mobilization and/or controlled physical activity during their ICU stay to mitigate loss of skeletal muscle mass and optimize anabolic effects of nutritional treatment. Once ICU or non-ICU patients are recovering from COVID-19, they should be checked for malnutrition and followed-up with dietary counseling by experienced professionals. This is especially true for older individuals, those with multiple comorbidities and those who were admitted at the ICU. There is a high risk for loss of muscle mass with ensuing malnutrition and sarcopenia among persons with obesity recovering from COVID-19. They should be encouraged to perform safe and adequate physical activities, including exercise programs, ideally individualized ones established by experienced professionals. Lastly, these individuals recovering from COVID-19 should resume or start multiprofessional support for appropriate treatment and nutritional management of obesity and related comorbidities and metabolic complications as soon as possible. In the light of possible worsening of nutritional status or worsening or new onset malnutrition during the course of COVID-19, treatment goals, metabolic profile, status of comorbidities, as well as any need for changes in dietary and lifestyle goals should be reassessed.
REFERENCES
- Barazzoni, R., Bischoff, S. C., Busetto, L., Cederholm, T., Chourdakis, M., Cuerda, C., Delzenne, N., Genton, L., Schneider, S., Singer, P., Boirie, Y., & endorsed by the ESPEN Council (2021). Nutritional management of individuals with obesity and COVID-19: ESPEN expert statements and practical guidance. Clinical nutrition (Edinburgh, Scotland), S0261-5614(21)00248-X. Advance online publication. [Link]
- Cederholm T, et al., GLIM criteria for the diagnosis of malnutrition − A consensus report from the global clinical nutrition community, Clinical Nutrition (2018), [Link]
- World Health Organization Western Pacific Region. The Asia-Pacific perspective: redefining obesity and its treatment [Internet] Geneva: World Health Organization; 2000. Available from: [Link]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults–The Evidence Report. National Institutes of Health. (1998). Obesity research, 6 Suppl 2, 51S–209S.
